Conversation with Mircea Sofonea: “In France, control of the epidemic remains fragile”
On May 3, we entered the first phase of a four-phase plan to ease lockdown restrictions. With the second phase, set to begin on May 19, restaurants, outdoor dining areas, cultural venues, and sports facilities are expected to reopen. On the eve of these easing measures, what is the current status of the pandemic?
Mircea T. Sofonea, University of Montpellier

What can we expect as the virus evolves, and what impact might this have on the strain on hospitals? Mircea Sofonea, associate professor of epidemiology and the evolution of infectious diseases at the University of Montpellier, provides the answers.
The Conversation: We've been through three lockdowns in a year. How does this latest one compare to the previous ones?
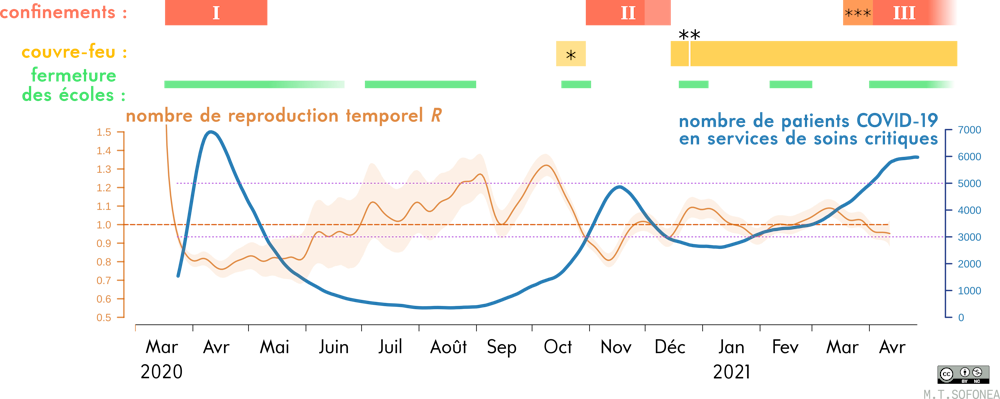
Mircea Sofonea: Based on hospital data and genetic analysis of samples collected in our country, it appears that the first wave of the COVID-19 pandemic in France began during the second half of January 2020.
In the spring of that same year, an initial strict eight-week lockdown had succeeded in reducing the number of new daily cases to 4,000 by the time restrictions were lifted. France then experienced a lull during the summer, before facing a second wave in the fall, which led to a second nationwide lockdown in October 2020—even though the benefits of early, region-specific measures were already well documented. This second lockdown was not sufficient, in terms of its intensity and duration, to bring the incidence back below 5,000 new (detected) cases per day—notably because viral circulation among children was underestimated, and due to the easing of restrictions associated with the end-of-year holidays.
See also:
What Do We Know About the Role of Schools in the COVID-19 Pandemic? Five Experts Weigh In
From that point on, the government opted for a strategy that differed from that of its neighbors in managing the pandemic, allowing for substantial circulation of the virus, accompanied by high hospital occupancy rates. In addition to this intermediate level of control, social restrictions, such as curfews, were maintained. This decision was motivated by the hope that there might be a “loophole” to exploit in order to minimize both the economic and public health impacts at every stage of the pandemic. This hope proved to be illusory, as subsequent events demonstrated.
Sofonea M. T., et al. (2021) Anaesthesia Critical Care & Pain Medicine, Author provided
This strategy was continued in early 2021, despite the emergence of the so-called “British” variant—which is more contagious—whose spread was documented relatively early on. As a result, a third nationwide lockdown had to be imposed on April 3. Schools were closed for three weeks (including two weeks of school vacation), and relative freedom of movement was maintained.
TC: Did this third lockdown achieve its intended goals?
MS: As we noted in an article recently published in *Anaesthesia Critical Care & Pain Medicine* (the official journal of the French Society of Anesthesia and Critical Care), a lockdown has two objectives: to cap hospital occupancy in order to prevent a deterioration in patient care, and to regain control of the epidemic by minimizing the incidence—in other words, by reducing the number of new cases per day to a level low enough to be managed through an intensive strategy of testing, contact tracing, and isolation.
Implemented late, this third lockdown was not as effective as the previous two (due in particular to the high transmissibility of the dominant variant, B.1.1.7). It was also relatively short. However, we know that the longer we wait to take action, the higher the levels of viral circulation and hospital occupancy will be, and therefore the longer it will take to return to acceptable levels in terms of controlling the epidemic (low incidence, low hospital occupancy). At the end of the second lockdown, hospital occupancy—particularly in critical care units, which had been under relentless strain for 14 months—had not returned to the low levels seen during the first lifting of restrictions.
This new lockdown has certainly achieved its primary objective—capping hospital occupancy: currently, there are approximately 5,600 COVID-19 patients in public intensive care units.
On the other hand, the second objective has not really been achieved: the reproduction number calculated three weeks after the start of the third lockdown was approximately 0.95—but it has since declined (Editor’s note: Also known as “effective R,” the reproduction number is an estimate, based on the last 7 days, of the average number of people infected by a single infected individual). After the first lockdown, this number had dropped to around 0.8 within two weeks—in kinetic terms, the decline in the epidemic during the first two weeks of the third lockdown was therefore more than three times slower.
Under these circumstances, it would take several more weeks to return to a level of 3,000 new cases per day, as was the case during the first easing of lockdown restrictions a year ago.
TC: Announcements have been made regarding the end of this third lockdown. What might happen next, according to your models?
MS: In a way, the course the pandemic has taken in the country since October has led us to a kind of impasse.
On the one hand, epidemic control is still too fragile and relies heavily on individual responsibility. On the other hand, we all want to return to our normal routines and our pre-pandemic lives; we are weary, if not exasperated, by the restrictions, and even maintaining them could lead to resistance and attempts to circumvent them.
The only option, therefore, seems to be accepting the morbidity and mortality toll caused by a third wave that is slowly subsiding. For it is important to remember that the public health challenge is not limited to deaths due to COVID-19 (all too often used as the sole metric), but also extends to quality of life after intensive care, long COVID, and conditions whose diagnosis and treatment were delayed by cancellations resulting from the rise of the third wave (particularly in Île-de-France and Hauts-de-France).
TC: But this time, the vaccine is available. And the warm weather is on its way…
Fortunately, vaccination coverage has a significant effect, but the current level is not yet high enough for it to stop the epidemic on its own. According to our model, which accounts for the increased transmissibility of variants but not for potential immune escape, achieving herd immunity would require vaccination coverage of 70% of the population (or more than 90% of the adult population); however, at present, we are at 25% for the first dose.
As for sunny days, they can help reduce transmission as long as they are accompanied by spending more time outdoors and in well-ventilated homes. However, if we look at the history of the reproduction number since the first lockdown was implemented, we see that there have been two peaks in transmissibility with a reproduction number above 1.3: in August and in October. Again, we cannot say that summer weather guarantees absolute control.
At social gatherings, even if most of the time is spent outdoors, a brief gathering indoors (in the kitchen) without masks still poses a risk of transmission. Crowded outdoor patios where people speak loudly (against a background of noise or commotion), shoulder to shoulder, also expose us to infectious aerosols, even though they dissipate much more quickly than indoors.
Ultimately, the situation in the coming weeks will once again depend on our collective adherence to preventive measures, combined with the three-pronged approach of testing, contact tracing, and isolation.
TC: With all these uncertainties, how can we assess what might happen?
MS: It is very difficult to make predictions beyond two weeks, given the uncertainties surrounding the combined effects of the various measures. However, we can draw on previous experiences with easing lockdown restrictions to explore scenarios, which then lead to projections based on assumptions.
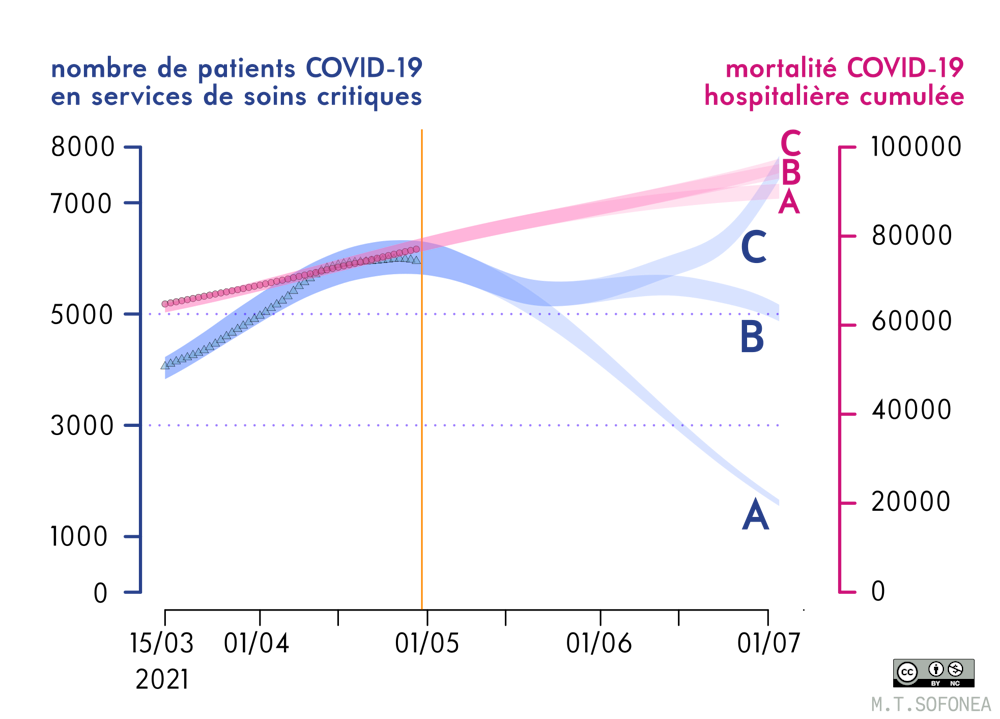
In the first scenario, if the contact rate (the number of contacts between people per unit of time) were to remain similar to that of October, the incidence rate would rise slightly before beginning a slow decline, mainly due to increased vaccination coverage. In this scenario, the number of patients in intensive care would not fall below 4,000 until July.
Sofonea M. T., et al. (2021) Anaesthesia Critical Care & Pain Medicine, Author provided
In the second scenario, if the contact rate were even just 10% higher than it was in October, the epidemic could experience a resurgence that would once again put intense strain on intensive care units, as early as mid-June, after reaching a low point in late May, with around 5,000 patients hospitalized in critical care.
TC: How did the other countries that were most successful in containing the outbreak go about it?
MS: The countries that fared best did everything they could to bring the outbreak under control as quickly as possible, and then resumed normal life: this is the case in South Korea, New Zealand, and Taiwan, for example. However, there’s no denying that they benefited from more favorable conditions.
Compared to countries that have aimed for elimination, it can be said that France has, since last summer, chosen to minimize the number of lockdown periods rather than the number of lockdown days, resulting in a suboptimal “stop-and-go” approach that has not minimized the spread of the virus. It is better to implement more lockdowns—but ones that are short and localized, as the New Zealanders did in Auckland (or the Chinese in Beijing, for example)—to break the chains of transmission very early on.
Furthermore, by failing to significantly reduce the incidence rate before relying on vaccination coverage to control the epidemic (as the United Kingdom, Portugal, and Denmark have done, for example), the possibility of local resurgences in early summer cannot be ruled out in France. Another disadvantage of vaccinating while the incidence is high (and viral diversity is therefore naturally greater) is that there is a greater risk of variants emerging that are better equipped to evade natural or vaccine-induced immunity. If vaccination takes place when the virus is circulating at very low levels, this risk is lower.![]()
Mircea T. Sofonea, Associate Professor of Epidemiology and the Evolution of Infectious Diseases, MIVEGEC Laboratory, University of Montpellier
This article is republished from The Conversation under a Creative Commons license. Readthe original article.