In France, mosquitoes also transmit the Usutu virus
The incident occurred two years ago, but scientists have only recently discovered that it was the first case of human infection with the Usutu virus in France. On November 10, 2016, a 39-year-old man was hospitalized for three days in the neurology department at Montpellier University Hospital due to sudden paralysis of half his face.
Yannick Simonin, University of Montpellier
The patient fully recovered within a few weeks, with no lasting effects. Subsequent tests showed that he had been infected with this virus.
It was the research conducted by our team of biologists from the University of Montpellier, Inserm, and the Montpellier University Hospital that led to an understanding of the cause of this man’s symptoms. We analyzed 666 cerebrospinal fluid samples collected from patients hospitalized in 2016 in Montpellier and Nîmes, as explained inthe article we have just published in the journal *Infectious Emerging Diseases*. Only one sample tested positive for the Usutu virus: his.
The most likely scenario is that this man was infected by a mosquito after it bit a bird, which serves as a reservoir for this virus. Transmitted to humans primarily by the Culex mosquito—which is common in France—this virus has been circulating in our country since at least 2015, according to a study by the French National Agency for Food, Environmental and Occupational Health & Safety (ANSES). Along with chikungunya, dengue, and West Nile virus, Usutu is now among the mosquito-borne viruses that have caused at least one indigenous case in France—that is, in a person who has not traveled abroad. While Usutu is not the most dangerous of these viruses that the French must learn to live with, it nonetheless deserves the attention of scientists and health authorities.
A name taken from a river in Swaziland, Africa
Until recently, the Usutu virus was virtually unknown. It has attracted the attention of the scientific community due to its widespread transmission in Europe. Usutu is an arbovirus belonging to the Flaviviridae family and the genus Flavivirus, which comprises more than 70 species.
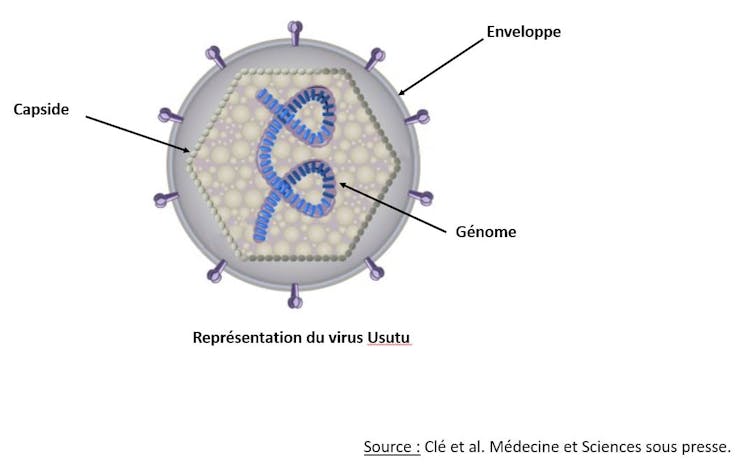
Clé et al. Medicine and Science, in press.
Among these are some of the most dangerous arboviruses for humans, such as the Zika virus, dengue virus, yellow fever virus, and West Nile virus. Usutu was named after the river of the same name located in Swaziland, a small African country that shares a border with South Africa. It was first identified there in 1959.
Little is known about Usutu’s target cells. Nevertheless, our team recently described its ability—like that of other flaviviruses—to infect cells of the nervous system in vitro (in the laboratory).
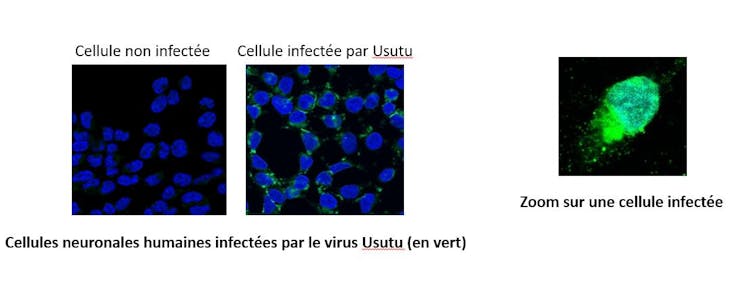
Salinas et al., PLoS Negl Trop Dis., September 5, 2017; 11(9): e0005913.
Birds as hosts, mosquitoes as vectors
The natural transmission cycle of Usutu is enzootic, meaning it is confined to a specific area. It primarily involves passerine birds (such as blackbirds and magpies) and strigiform birds (such as Lapland owls) as “amplifier” hosts, meaning they facilitate the active replication of the virus. Ornithophilous mosquitoes (which bite birds) serve as vectors for transmission to humans.
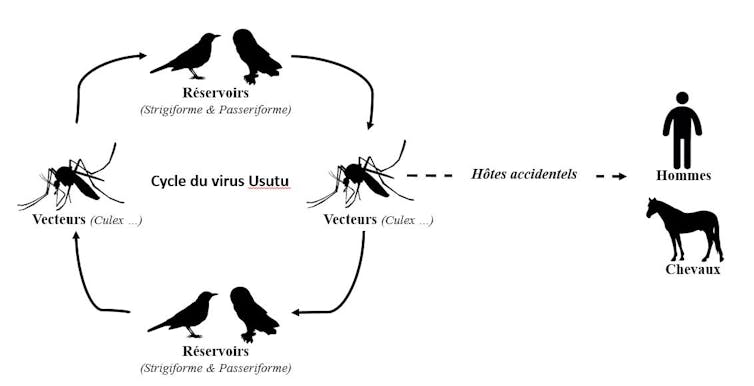
Clé et al. Medicine and Science, in press.
Various studies have demonstrated the involvement of several mosquito species in sustaining the Usutu cycle within the avifauna—that is, among birds inhabiting the same area. The virus has thus been isolated in the following mosquito species: Aedes albopictus (better known as the tiger mosquito), Aedes caspiuis, Anopheles maculipennis, Culex quinquefasciatus, Culex perexiguus, Culex perfuscus, Coquillettidia aurites, Mansonia africana, and Culex pipiens. These species are bird-biting but also bite humans.
Mosquitoes transmit the virus to humans as well as to horses. These species are susceptible to Usutu but are considered accidental hosts and epidemiological “dead ends”—that is, they cannot transmit the virus to other members of their own species.
High bird mortality
Usutu has also been detected in numerous bird species. Several migratory species are believed to be responsible for introducing Usutu to Europe, while others are thought to be responsible for its spread. Among the species susceptible to Usutu infection, blackbirds ( Turdus merula ) have the highest mortality rate.
Central nervous system disorders have been reported in birds infected with Usutu. These birds exhibit lethargy, disorientation, impaired motor coordination, and weight loss. Postmortem examination frequently revealed inflammation of the liver (hepatomegaly) and the spleen (splenomegaly).
Lesions have also been reported in the heart, liver, kidneys, spleen, and brain of infected birds. These observations show that Usutu can be highly pathogenic in bird populations due to its replication and virulence in a wide range of tissues and organs. Usutu thus causes significant mortality among birds in various regions of Europe.
A virus first discovered in Europe in 2001
The virus was first detected in Europe in 2001, in Austria, in dead birds. It was subsequently reported in many European countries, in mosquitoes or birds.
In 2015, France also detected this virus in common blackbirds, following a rise in mortality rates in the Haut-Rhin and Rhône departments, which was analyzed by ANSES and the National Office for Hunting and Wildlife (ONCFS).
Furthermore, it has since been established that Usutu has been circulating among Culex pipiens mosquitoes in the Camargue since at least 2015. During the summer of 2016, a major Usutu outbreak affecting birds was again recorded in Europe, with widespread viral activity in Belgium, Germany, France, and, for the first time, the Netherlands. This phenomenon highlights not only the continued geographic spread of Usutu but also the emergence of new ecological niches.
The recurrence of Usutu infection in various European countries suggests a persistent transmission cycle in the affected areas, either through overwintering mosquitoes (the cold slows their metabolism, and they remain inactive until spring) or through repeated reintroduction of the virus by migratory birds from Africa.
Symptoms that need to be better characterized
The risk of animal-to-human transmission associated with Usutu was first described in Africa. The first human case was reported in the Central African Republic in the 1980s, and the second in Burkina Faso in 2004. In both cases, symptoms were moderate, including a rash and mild liver involvement.
In Europe, there have been 28 cases of acute human infection with Usutu to date, mainly in Italy. In addition, more than 70 people with antibodies against this virus have been identified, indicating that these individuals have been exposed to the pathogen. Human infection is likely to be asymptomatic in most cases, or to present with mild clinical symptoms. However, neurological complications such as encephalitis (inflammation of the encephalon, the part of the brain located within the skull) or meningoencephalitis (inflammation of the encephalon and the meninges, the membranes surrounding it) have been reported, totaling about 15 cases in Europe.
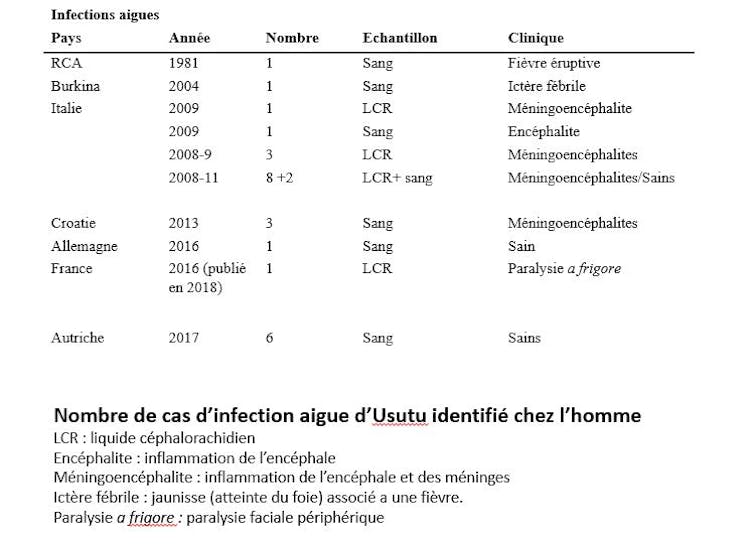
Clé et al. Medicine and Science, in press.
Our team’s description of the unusual occurrence of facial paralysis in the first French case suggests that the full range of symptoms associated with Usutu virus infections is not yet fully understood.
A virus whose range is expanding
The recent history of outbreaks of other arboviruses calls for the scientific community to exercise the utmost vigilance regarding the Usutu virus. Its range now extends to a large number of European countries. Epizootics causing avian mortality are frequent. Genetically very different strains are circulating simultaneously. All of these are warning signs.
Although they are too few in number, a few seroprevalence studies (measuring the presence of antibodies against the virus in the blood) support the hypothesis that humans are at greater risk of Usutu infection than is commonly believed.
![]() Our understanding of the pathophysiology of this emerging virus is currently very limited. Ongoing research is focused in particular on gaining a better understanding of its biology and the mechanisms associated with neurological damage. Research efforts are therefore being accompanied by surveillance measures and prevention should be implemented in France, in the areas most at risk.
Our understanding of the pathophysiology of this emerging virus is currently very limited. Ongoing research is focused in particular on gaining a better understanding of its biology and the mechanisms associated with neurological damage. Research efforts are therefore being accompanied by surveillance measures and prevention should be implemented in France, in the areas most at risk.
Yannick Simonin, Inserm researcher and associate professor of infectious disease control, University of Montpellier
The original version of this article was published on The Conversation.